Read in Chinese
Speakers:
Wang Hesheng, vice minister of the National Health Commission (NHC) and administrator of the National Administration of Disease Control and Prevention
Zeng Yixin, vice minister of the NHC
Jiao Yahui, director of the Bureau of Medical Administration of the NHC
Chairperson:
Shou Xiaoli, deputy director general of the Press Bureau of the State Council Information Office (SCIO) and spokesperson of the SCIO
Date:
March 18, 2022
Shou Xiaoli:
Ladies and gentlemen, good afternoon. Welcome to this press conference held by the State Council Information Office (SCIO). To implement the major directives of the Central Committee of the Communist Party of China (CPC) on COVID-19 prevention and control, today the SCIO is holding a press conference on the rigorous COVID-19 response, and we will also answer your questions. We are joined by Mr. Wang Hesheng, vice minister of the National Health Commission (NHC) and administrator of the National Administration of Disease Control and Prevention; Mr. Zeng Yixin, vice minister of the NHC; and Ms. Jiao Yahui, director of the Bureau of Medical Administration of the NHC.
Now, I will give the floor to Mr. Wang Hesheng.
Wang Hesheng:
Friends from the media, good afternoon. Thank you for your interest in and support for the COVID-19 prevention and control work. First, I will introduce the current priorities of the COVID-19 response, and then my colleagues and I will take your questions.
The CPC Central Committee and the State Council attach great importance to COVID-19 prevention and control. General Secretary Xi Jinping has taken personal command, planned the response, and made a series of important instructions. He has emphasized adherence to the overall strategy of "preventing inbound cases and domestic resurgence" and the dynamic zero-COVID approach, as well as the need to coordinate the COVID-19 response with economic and social development.
Yesterday, on March 17, General Secretary Xi Jinping presided over a meeting of the Standing Committee of the Political Bureau of the CPC Central Committee to analyze the latest COVID-19 developments and arrange for better and more stringent epidemic control measures. General Secretary Xi Jinping emphasized that victory comes from perseverance, and all local authorities and government departments must be fully aware of the complex, arduous and enduring nature of COVID-19 control both at home and abroad, further social mobilization, build consensus, proceed with greater confidence and perseverance, and carry out all the epidemic control work in a more solid and meticulous manner. He emphasized the need to always put people and their lives first, adhere to the dynamic zero-COVID approach with science-based and targeted measures, and contain the spread of the virus as soon as possible. He said that efforts must be taken to make the epidemic response more science-based and targeted and keep optimizing the response measures. He also called for maintaining strategic focus, pursuing progress while ensuring stability, coordinating the COVID-19 response with economic and social development, adopting more effective measures, striving to achieve the best results in epidemic control with minimum costs, and minimizing the epidemic's impact on the economic and social development.
The NHC and the National Administration of Disease Control and Prevention have been earnestly implementing General Secretary Xi Jinping's important instructions. In response to multiple local case clusters in parts of China, we have worked with relevant authorities to strengthen guidance for key regions. We have worked to ensure "early detection, reporting, isolation and treatment," implement stringent epidemic prevention and control, and resolutely take more effective and targeted measures. These steps are aimed at suppressing local outbreaks as soon as possible and providing an enabling environment for people's lives and economic and social development.
First, we have worked swiftly on the emergency COVID-19 response. Recently, China has seen cluster infections spreading widely and occurring frequently in multiple regions. The comprehensive working group under the State Council's inter-agency task force immediately sent national working groups to provinces including Jilin, Shandong, Guangdong and Heilongjiang to guide their COVID-19 response. The groups worked with local authorities to assess the COVID-19 situation, develop response measures, accelerate screening through nucleic acid testing, investigations and regional checks, ensure "early detection, reporting, isolation and treatment," provide the best possible treatment for patients, and curb the spread of the virus.
Second, we have consolidated the defense line against inbound infections. We worked to ensure sound prevention for people, objects and environments, tighten personnel management at points of entry, implement strict closed-loop management, and increase the frequency of nucleic acid tests; guard against risks from imported cold-chain food and high-risk non-cold-chain objects; step up the management of border areas and points of entry, and intensify the crackdown on illegal entries and exits. We worked vigorously with our land neighbors to build a joint prevention and control mechanism and ensure sound epidemic prevention and customs clearance for cargo at border areas.
Third, we have increased capacity for preventing, controlling and handling infections. We improved COVID-19 response plans on monitoring, epidemiological investigation, quarantine for medical observation, community (village)-based epidemic prevention and control, sample collection and testing. We worked to ensure those who test positive are reported and investigated immediately and control measures are taken before screening. We regulated work on the screening of people at risk, the management of close contacts, and identification of risk areas. We attached equal importance to both traditional Chinese medicine and Western medicine and provided standard and regulated treatment. We worked to guarantee the implementation of the first consultation responsibility system and strengthen prevention of hospital-acquired infections. We carried out record-based management of more than 7,000 fever clinics and over 800 designated hospitals. We also enhanced our testing capacity, with national testing capacity reaching over 40 million samples per day.
Fourth, we work hard to implement vaccination programs. In line with the plans of the State Council joint prevention and control mechanism, we have guided local authorities to step up COVID-19 vaccination and booster vaccination efforts in a proactive, prudent, and orderly manner and further raise the overall vaccination rates.
Our achievements in epidemic prevention and control are not easily attained, and it is important to fully recognize their value. Next, we will work together with relevant departments to fully implement the decisions and plans of the CPC Central Committee and the State Council and further step up our efforts in key epidemic control tasks.
First, we will bring local cluster infections under control as soon as possible. We will guide key regions to accelerate nucleic acid testing and speed up identification, epidemiological investigation, and management of at-risk groups so as to achieve dynamic zero-COVID in communities as soon as possible.
Second, we will reinforce the line of defense against imported cases. We will adopt remote prevention and control measures on inbound arrivals, prioritize close-loop management, and expand monitoring coverage of key groups. We will also see that special working teams at port-of-entry areas fulfill their responsibilities for COVID-19 control by stepping up patrols along river banks and coastlines and strengthening the deployment of anti-epidemic personnel.
Third, we will strengthen routine epidemic control and management in key places and key regions. Guidance will be given to schools, nursing homes, detention centers, passenger terminals, shopping malls, supermarkets, and other key venues and densely populated places, as well as cold-chain workers, shopping mall and supermarket staff, logistics workers, and people from other key sectors, for them to strictly implement anti-epidemic measures.
Fourth, we will make the epidemic response more science-based and targeted. We will strictly implement pre-examination triage, and the first consultation responsibility system. We will also improve the mechanism for issuing early warnings through multiple channels and promote a monitoring model that uses antigen testing for earlier detection and the nucleic acid test for diagnosis. Guidance will be given to local authorities to ensure that their epidemic control work will be more science-based and targeted, minimizing the epidemic's impact on economic and social development.
That's all for my introduction. Thank you.
Shou Xiaoli:
Thank you for your introduction, Mr. Wang. Let's move on to the question-and-answer session. Please identify the media outlet you represent before asking a question. Now the floor is open for questions.
_ueditor_page_break_tag_
China Media Group:
The recent infections feature outbreaks in multiple regions, a wide spread of the virus, and a large number of confirmed cases. What is your assessment of this round of infections? What features have you found from virus origin tracing? What do you think is the reason for the recent resurgence? Thank you.
Wang Hesheng:
Thank you. Now I will answer your questions. Just as you said, we have indeed seen recent infections spreading widely and occurring frequently in multiple regions. There are four main reasons:
First, since December 2021, the world has witnessed the fourth pandemic peak of COVID-19, which has lasted for 11 consecutive weeks up to now, with more than 10 million cases reported each week. These figures show that the world is still at a pandemic peak. Since the start of this year, in particular, the virus has spread rapidly in our neighboring countries and regions, producing an increasing "pressure difference" in COVID-19 spread between China and its neighbors. In the first two months of this year, the average number of daily imported infections reached 91 cases, far more than 22 cases in 2020 and 32 cases in 2021. In March 2022, the average number of daily imported infections exceeded 200, with the highest daily number exceeding 300 cases. All these indicate a significant increase in the pressure caused by the recently imported infections.
Second, the Omicron variant of the coronavirus that is now dominant worldwide, especially the Omicron BA.2 sub-variant, is more contagious and less detectable than other strains. So this makes it harder to detect the virus at an early stage. When discovered, the Omicron variant may have already spread to a wide area. And this means that it has become more difficult for us to handle and control the coronavirus.
Third, in late February, Spring Festival ended, the spring semester began, and companies and workers resumed normal work, which brought a massive flow of population. And there was also an increase in gatherings, such as meetings, training activities, weddings, and funerals. All of these have magnified and amplified the spread of COVID-19, leading to the fast spread of coronavirus and even the transmission across regions.
Fourth, some may think the Omicron variant appears to have relatively mild symptoms and is no different from the flu, then they relax their vigilance in guarding against the coronavirus and are not fully prepared to respond to COVID-19, lowering requirements for regular containment measures and emergency responses.
According to analyses and assessments by experts, this wave of global COVID-19 outbreak is still at a high level and will not come to an end soon. China will continue to face a situation where Omicron-dominated infections may occur in multiple locations simultaneously. It means that epidemic prevention and control will be even more serious and complex.
Epidemiological tracing results also show that the recent cluster infections in multiple regions of China were all caused by inbound cases. In addition, most of the people infected with the Omicron variant present mild symptoms or are asymptomatic, so it is hard to detect the source of the virus and the means of transmission vary significantly. We have discovered multiple transmission routes in different regions and found the source of the coronavirus diverse and complex. This brings huge challenges to the epidemiological tracing work and COVID-19 response.
The characteristics of this wave of the coronavirus outbreak require us to further increase sensitivity in our monitoring and early warning efforts, improve the multi-point trigger mechanism for monitoring, and effectively improve our capacity to detect the coronavirus at an early stage. Thanks.
_ueditor_page_break_tag_
Kyodo News:
We know that China's dynamic zero-COVID policy has been successful. However, the recent COVID-19 containment measures may restrict China's manufacturing sector and consumption and make it difficult to communicate with the overseas market, which triggers worries from foreign-invested enterprises. Will the dynamic zero-COVID policy see any changes in the first half of this year? Thanks.
Wang Hesheng:
Thank you, I will answer your question. Since the outbreaks, under the strong leadership of the CPC Central Committee with Comrade Xi Jinping at its core, China has always put people's lives and health first. We have strengthened our COVID-19 response on all fronts, which delivered outstanding performance and protected the safety and health of the public to the utmost.
The dynamic zero-COVID approach was put forward under the principle of preventing the coronavirus from entering the country and stemming its domestic resurgence, and is based on summarizing our experiences and learning from lessons. The approach requires us to detect cases at an early stage, contain small outbreaks, and focus on work at a primary level so as to improve our COVID-19 response and our capacity to detect COVID-19 cases early. We act swiftly to detect the people infected and outbreaks at an early stage. When discovered, we take immediate actions to cut off virus transmission so as to reduce infections and achieve dynamic zero infection. The goal of the dynamic zero-COVID approach is to bring the epidemic under control in the shortest possible time with a minimum cost to society. The essence of the approach is to act swiftly and take targeted measures to prevent and control the coronavirus. When we say "act swiftly," we mean to detect and handle the virus rapidly and cut off its transmission quickly. When we say "targeted measures," we mean that the measures are put in place throughout all links, including epidemiological tracing, quarantine, community-level disease prevention and control, and clinical treatment.
We should be aware that China has well balanced COVID-19 prevention and control and its economic and social development. The country has become the world's only major economy to register positive growth. This progress did not come easily. It has been proven that China's practice in responding to COVID-19 has safeguarded people's lives and health and ensured economic growth.
In fact, COVID-19 has affected the economic and social development of all countries across the world to different degrees. But the results of different COVID-19 response strategies and measures may vary in easing and controlling those negative impacts. When assessing the impact on the economy or the cost of prevention and control measures, we should figure out what kind of impacts are caused by COVID-19 itself, what is brought by economic development, and what impacts the COVID-19 response strategy and containment measures will have. I don't think we can solely owe the economic impacts to the COVID-19 response strategy and epidemic prevention and control measures.
Second, when assessing the cost and effect of COVID-19 response measures, we should take a scientific approach. They can be assessed in four dimensions.
The first is the cost and result of prevention and control; that is, how much cost is spent, how many infections, severe cases and deaths are reduced. I think the prevention and control concept of our Party and government is that people come first, life comes first, and that we must protect the lives and health of the people to the greatest extent possible. Therefore, we can see that the total number of infected individuals, the number of cases, the number of severe cases, and the number of deaths in China are very small, which shows that the cost-effectiveness ratio of prevention and control in China is high.
The second is cost-efficiency; that is, the speed with which the pandemic can be contained and extinguished. China's prevention and control work is basically within the one or two longest incubation periods to quickly deal with and quickly extinguish the pandemic, which shows that the cost-efficiency ratio is high.
The third is cost-utility; that is, through the dynamic zero-COVID approach and precise prevention and control. China has ensured the normal production and life of the vast majority of regions and people, reducing inconveniences caused by the pandemic and even reducing psychological and other health problems. This shows that, by limiting the normal activities of a very small portion of people and controlling the population movements within a very small part of the country, we ensured the normal production and life of the broadest areas and people.
The fourth is cost-benefit; that is, the economic benefits achieved at the cost of prevention and control. In this regard, the key is to look at the big picture and do not only focus on the current situation. It is neither comprehensive nor objective to calculate cost-benefit only based on the costs incurred at the location and time of an outbreak. We should take the entire country as a whole and consider the general benefits to the entire economy, the entire society and the overall well-being of the people.
Facts have proven that the practice of the dynamic zero-COVID approach is in line with China's national conditions and scientific laws. The approach is correct and the result is good. Although the prevention and control measures of the dynamic zero-COVID approach will have some impacts on production and life in some areas, these impacts are short-term and limited in scope. We should say, any prevention and control measures will have certain costs, but for protecting people's lives and health, these costs are worth it. Here I would like to express my special thanks to our broad masses of the people for their understanding, support, and cooperation with the pandemic prevention work.
China's anti-pandemic practice shows that adhering to the dynamic zero-COVID approach is the current pandemic defense line that we as a great country with a population of more than 1.4 billion must guard. This is our best way to embody the idea of "people first" and "life first". This is also the biggest contribution to the international fight against the pandemic. Thank you.
_ueditor_page_break_tag_
Southern Metropolis Daily:
What is the current progress of vaccination in China? What is the difference between sequential booster immunizations using vaccines from different technical routes and homologous booster immunizations using vaccines from the same technical route? What is the next step for implementation? Thank you.
Wang Hesheng:
We'd like Mr. Zeng Yixin to answer these questions.
Zeng Yixin:
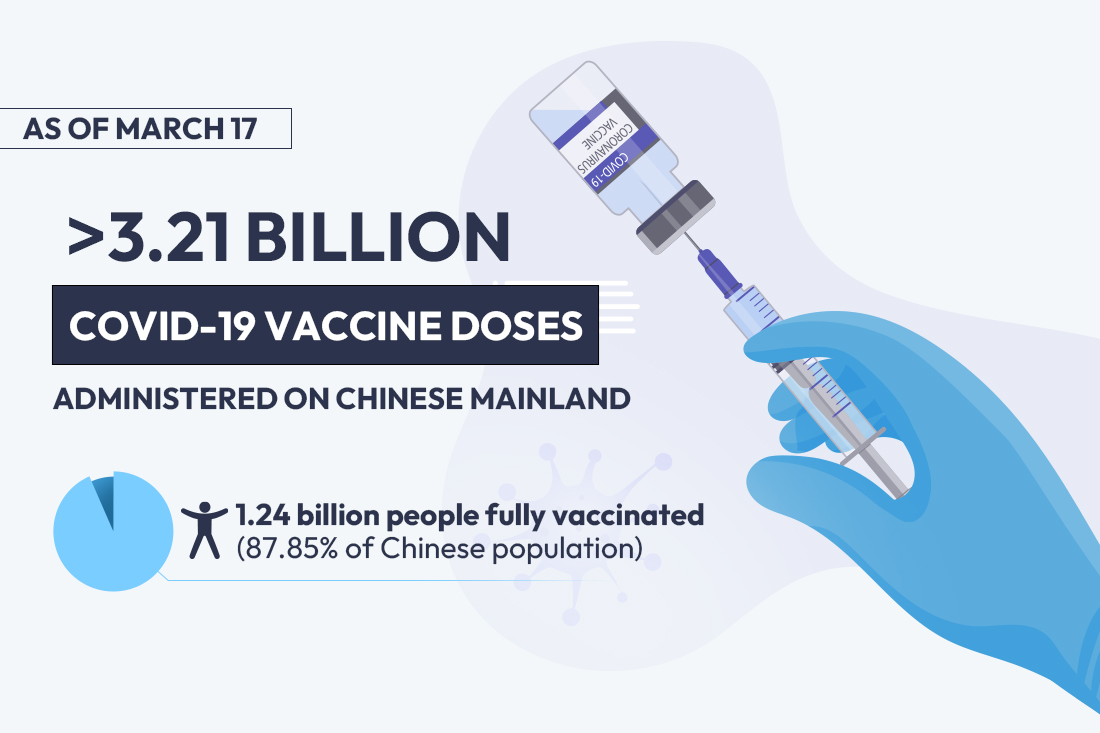
Thank you for your interest in vaccinations. According to the decision-making and deployment of the CPC Central Committee and the State Council, and the unified arrangements of the Joint Prevention and Control Mechanism of the State Council, all parts of the country are steadily and orderly advancing the vaccination of the COVID-19 vaccines. As of March 17, China has reported more than 3.21 billion doses of vaccinations and the total number of people vaccinated is more than 1.27 billion, among whom more than 1.24 billion people have completed the full course of vaccination, accounting for 87.85% of the total population, while 644.68 million people completed booster immunizations.
According to the pandemic situation, the needs of prevention and control, and the progress of vaccine development and use in China, starting from October 2021, the Joint Prevention and Control Mechanism of the State Council launched the work for COVID-19 vaccine homologous booster immunizations. That is to say, the same vaccine used for the full course of vaccination will also be used for the booster shot. We call this the "homologous booster." Recently, we have made some additional supplements and improvements to the COVID-19 vaccine booster immunization strategy, adding sequential booster immunization. The sequential booster immunization means that the booster immunization can choose a vaccine different from the original basic immunization. What is currently approved is that on the basis of inactivated vaccines, the vaccination can be boosted with adenovirus vector vaccines, or it can be boosted with recombinant protein vaccines. Next, we will probably add more options based on the progress of vaccine research and development in China.
According to the current policy, all people who meet the requirements for booster immunizations can receive booster immunizations six months after the full course of basic immunization. The booster immunization includes homologous or sequential immunization. For eligible populations, choosing one immunization option is enough for each person, be it either homologous or sequential vaccination. You all are also concerned about the differences between homologous and sequential vaccinations. Some relevant studies have been carried out at home and abroad on this issue, and some reports have been published. These studies show that both the homologous booster and sequential booster can significantly improve the immune protective efficacy, which is very clear. I just said that more than 600 million doses of booster immunization have been completed in China. Since the sequential booster immunization was carried out a little later, of the more than 600 million doses, most are homologous. However, from the adverse reaction data we have collected, there is no significant difference in adverse reactions between the two methods, so please feel free to vaccinate. We hope that people who meet the requirements for booster immunization, especially the elderly and those with underlying diseases, can take the initiative to vaccinate and get vaccinated in a timely manner so as to increase the protection of their own health and contribute to the pandemic prevention of the whole society. Thank you.
_ueditor_page_break_tag_
Red Star News:
The NHC has released the ninth version of the COVID-19 diagnosis and treatment guidelines, making important adjustments in the management of people with mild COVID-19 infections and the cycle threshold value of a nucleic acid test. What are the reasons for the adjustments? Does it mean that prevention and control measures have been relaxed? Is it necessary for all localities to continue to implement strict prevention and control measures?
Jiao Yahui:
Thanks for your questions. First, I would like to make it clear that revisions to China's COVID-19 diagnosis and treatment guidelines do not mean relaxed prevention and control measures. All localities should continue to carry out COVID-19 prevention and control work with caution constantly. The revisions are based on our country's anti-epidemic experience over the past two years, especially the observation and research of clinical cases infected with the Delta and Omicron variants. The main adjustments involve the detection and reporting of cases and the adding of antigen testing to form the "antigen test plus nucleic acid test" tactic. In addition, we proposed classified treatment. We have also made adjustments to antiviral treatment, TCM treatment, criteria for being released from isolation and discharged from hospitals, and management following discharge. The adjustments are made in accordance with General Secretary Xi Jinping's important instructions to make the COVID-19 response more scientific and targeted, and achieve maximum effect in prevention and control with minimum cost.
I would like to give a detailed explanation on changes to the admission of cases. In terms of classified treatment, people with mild COVID-19 infections will be placed at centralized isolation facilities rather than in designated hospitals, according to the latest version of the guidelines. Mild, severe, and critical cases, as well as cases with other high risks, will be admitted to designated hospitals. In other words, asymptomatic and mild cases will be placed in centralized isolation. Here I want to clarify that centralized isolation facilities for asymptomatic and mild cases must be strictly separated from those designated for close contacts and overseas travelers because mild and asymptomatic cases have positive nucleic acid test results, while close contracts usually have negative nucleic acid test results, so isolation facilities for them must be strictly separated.
In response to the pandemic, some regions use special isolation facilities, such as Shandong province and Jilin province, where temporary treatment centers have been built. That doesn't mean that people with mild COVID-19 infections and asymptomatic cases placed in centralized isolation will go uncared. The revised guidelines require that the centralized isolation facilities where these cases are treated should also be staffed with medical personnel. What are the duties of those medical personnel? On the one hand, they should provide therapies to the mild cases, such as cases with symptoms of nasal obstruction, a cough, and fever. On the other hand, they should monitor the patients' conditions. Based on our practice, about 95 percent of patients in the latest outbreak are asymptomatic or only show mild symptoms. Although there are fewer treatment and intervention measures for them, it does not mean that we will leave them unattended. If their condition worsens, they will be timely transferred to designated hospitals for further treatment.
The other thing that people are concerned about is the CT (cycle threshold) value — part of the discharge criteria. In the ninth version of the diagnosis and treatment plan, we proposed that patients can be discharged from hospitals or centralized isolation when their two consecutive CT values are both 35 or above with at least 24 hours between the two tests and that the COVID-19 symptoms relieved, with some hospitalization-required symptoms gone. The adjustment is also based on our practical research. Research showed that the live virus cannot be isolated from samples of convalescent patients whose CT value is 35 and above, meaning that these patients are no longer infectious. Therefore, such patients can be discharged from hospitals and return home. These adjustments have been made to improve the utilization efficiency of medical resources. For one thing, we can concentrate in-need cases in hospitals to ensure effective medical treatment. For another, it also leaves us more medical resources to provide normal medical services for the public. The adjustment has fully embodied implementing the principle of putting the people and their lives first.
As for post-discharge management, we changed the previous 14-day isolation into seven-day health monitoring at home. Thus, the adjustments made to the latest diagnosis and treatment plan does not mean the pandemic prevention and control policies have been relaxed. Instead, they are more scientific, precise, and targeted. Thank you.
_ueditor_page_break_tag_
Bloomberg News:
I have two questions. One of the biggest impacts the dynamic zero-COVID policy has on the economy is that factories have to shut down and people have to quarantine for long periods. What can the government do to reduce that impact? Do you have any plans to introduce foreign vaccines or other foreign medicines to aid with the treatment of coronavirus? Thank you.
Wang Hesheng:
I'll answer these questions. First, thanks for your attention. Since the outbreak of COVID-19, the NHC and the National Administration of Disease Prevention and Control have resolutely implemented the decisions and arrangements made by the CPC Central Committee and the State Council, actively guided the localities to strengthen scientific prevention and control to take targeted measures, and firmly adhered to the overall strategy of preventing case imports and domestic resurgence as well as the general dynamic zero-COVID policy. With our continuously deepening understanding of how the novel coronavirus behaves, our anti-pandemic policies and measures have been consistently adjusted and improved in accordance with the changing epidemic situation and actual needs of the prevention and control work so as to make the work more scientific and accurate.
Since the anti-epidemic work entered the dynamic zero-COVID stage of targeted prevention and control across the whole chain, we have focused on early detection of sporadic cases to enhance the capacity of epidemic prevention and control and early spotting. Our work is mainly carried out in the following aspects:
First is to highlight prevention and improve the ability to prevent case import. We issued the Notice on Strengthening COVID-19 Prevention and Control in Port Cities and put forward clear requirements from multiple aspects to further rationalize mechanisms and clarify responsibilities. The aspects include improving the pandemic prevention and control mechanism in port cities; ameliorating the epidemic monitoring and early warning system; strengthening land and maritime border control; ensuring personal protection and closed-loop management of personnel in high-risk positions; enhancing prevention and control of each link of the cold chain; standardizing the monitoring, disinfection, and disposal of high-risk articles and environment at ports; increasing the capability of epidemic prevention, control, and handling; and securing people's livelihood.
Second is to emphasize early detection. We have further ensured that all those in need are tested, and made efforts to increase the frequency of nucleic acid tests and health monitoring of personnel working in port-of-entry areas, centralized isolation sites, designated medical institutions, and other key areas. We have fully leveraged the sentinel role of fever clinics, implemented the first consultation responsibility system, and regulated the reception and treatment procedures for patients with fever in individual clinics and community-level medical institutions. We have set up multi-channel and multi-spot trigger mechanisms in pharmacies, educational institutions, and community-level medical institutions, among others.
Third is to underline real results and upgrade the preparedness for dealing with the pandemic. All localities have been required to establish and maintain an emergency response command mechanism during both normal and emergency periods and apply the horizontal management model. At the national level, we have set up 16 national expert teams of epidemiological investigation responsible for eight regions nationwide. All localities have been required to set up sufficient epidemiological investigation teams composed of various departments of health, disease control, public security, and industry and information technology, and carry out exercises and training to effectively improve the epidemiological investigation capacity. We have also demanded that local governments effectively enhance the reserve capacity of nucleic acid test teams and coordinate and allocate resources to ensure that the nucleic acid test tasks are fully completed within a specified time.
Fourth is to accentuate speed and boost early handling of the pandemic. In the "golden 24 hours" after the detection of positive cases, while the positive samples in the preliminary screening are retested, emergency preparedness including epidemiological investigation, nucleic acid test, quarantine site arrangement, and community management and control will be simultaneously activated in accordance with the principle of reporting any positive case immediately, conducting investigation immediately after receiving the report, and controlling first before screening. We have ensured that multiple tasks of command system construction, nucleic acid test, isolation, medical treatment, and press release can be carried out in parallel.
Fifth is to underscore "strictness" by intensifying installation and management over designated hospitals. We have strengthened prevention and control over hospital infections, and reinforced installation and management over fever clinics, making sure that all hardware facilities meet the requirements for the prevention and control of respiratory infectious diseases. We have strictly implemented closed-loop management over the staff working at those fever clinics which receive high-risk groups, including fever patients from overseas and from medium-high risk areas and centralized quarantine locations in China. We have strengthened installation and management over designated hospitals, reinforced equipment and training over the prevention and control personnel against hospital infections, intensified screenings of medical workers before entering isolation wards, and earnestly put every prevention and control measure against hospital infections in place.
Next, the NHC and the National Administration of Disease Control and Prevention will jointly work with other relevant departments to conduct training and drills on a regular basis to improve practical emergency response abilities and multi-department collaboration abilities, and intensify risk monitoring and screening at key links. We have to prevent misinterpretation of policies, one-size-fits-all solutions, excessive implementation of policies, and other problems at local level while ensuring the full implementation of all measures, in a bid to create a sound environment to ensure people's wellbeing and promote economic and social development.
Regarding the question raised by this journalist on whether more foreign-developed vaccines and medicines will be introduced, I suggest you consult relevant departments. Thank you.
_ueditor_page_break_tag_
China Daily:
As Ms. Jiao mentioned, according to the ninth edition of China's COVID-19 diagnosis and treatment guidelines, recovered patients only need to monitor their condition at home for seven days after being discharged from quarantine locations or hospital, instead of conducting health monitoring and 14-day quarantine after being discharged from hospital. Could you please tell us the reasons for those modifications?
Jiao Yahui:
Thank you for your question. As we mentioned before, relevant studies have shown that the live virus can not be separated from samples if a patient's cycle threshold value is greater than or equal to 35. Given that, we have made such a modification. First, it is no longer contagious when the cycle threshold value is greater than or equal to 35. On the other hand, given on our study on reconfirmed positive cases in China, the epidemiological survey has demonstrated that those cases had not caused any transmissions or infections. Therefore, patients can be discharged from hospital when their cycle threshold values reach 35.
Second, the previous requirement that patients should spend 14 days in centralized quarantine or go to rehabilitation hospitals was based on our general experience. Now that we have proved it's non-infectious, it's reasonable to adopt at-home isolation and monitoring rather than centralized quarantine. Another adjustment is the change from 14 days to seven days. According to hospitals' observation on recovered patients infected with the Delta variant as well as those infected with the Omicron variant, their body functions can recover within seven days basically; thus, the time has been shortened from 14 days to seven days. Given our observations, research, and analysis of clinically diagnosed cases, we cut the time and adopted at-home isolation instead of centralized quarantine. Notably, in spite of staying at home, the patients still have to strictly implement health monitoring. Thank you.
_ueditor_page_break_tag_
New York Times:
Other countries and territories have found the elderly are the most vulnerable, and the only reliable way to protect them is through vaccination. What percentage of people in China who are 80 or older have had one vaccine, or have had two vaccines, or have had three vaccines for the coronavirus? And what are you doing to encourage these elderly people to be vaccinated fully if they have not already received two or three vaccines? Thank you.
Zeng Yixin:
It's a problem of great importance. The Joint Prevention and Control Mechanism of the State Council has always attached great significance to promoting vaccination among the elderly population in China by repeatedly making arrangements and plans. Additionally, the local departments have actively taken multiple measures to boost the vaccination rate among the elderly. You only mentioned people older than 80; I will introduce the general vaccination situation of people who are 60 or older. As of March 17, for people aged 60 to 69, the first dose rate, the full vaccination rate, and the booster vaccination rate hit 88.8%, 86.6%, and 56.4%, respectively. Among people aged 70 to 79, the numbers are 86.1%, 81.7%, and 48.4%, respectively. As for the group who are 80 or older, which you are mostly concerned, those three figures are 58.8%, 50.7%, and 19.7%, respectively. Generally speaking, of the 264 million people aged 60 or older, 211.76 million have been fully vaccinated, which means there are still 52 million people who have not received full vaccination. Among those, those aged 80 or older account for the largest proportion as their full vaccination rate and booster vaccination rate are a mere 50.7% and 19.7%, respectively. Both are relatively low percentages. As for the elderly, full vaccination and booster vaccination are of great importance, especially for people aged 80 or older. Therefore, we will step up efforts to vigorously promote vaccination among the elderly.
The immune system of the seniors is weaker than that of the young, and most of them have various underlying medical conditions. Once infected with the coronavirus, the risk of severe illness and death is much higher than that of the young. As we all know, there have been many clusters in China since last year, but very few of the infected became seriously ill. In particular, in the cases caused by the Omicron variant, the proportion of severe cases is even fewer. However, in the Yangzhou cluster outbreak that was caused by the Delta variant in August last year, the elderly cases accounted for a high proportion and thus more severe cases were found. There was a total of 1,388 cases in Yangzhou, of which 67 severe cases were among the elderly over 60 years old. Because there are many elderly people, the incidence of severe cases is also relatively high. Among the 1,388 cases, the proportion of people who had a complete course of vaccines was 38%. Among the 67 severe cases, 65 cases were not vaccinated or did not complete the full course of vaccination. In the recent Hong Kong outbreak, it is reported that the mortality rate of vaccinated people is 0.04%, and the mortality rate of those who have not been vaccinated or not fully vaccinated is 1.25%, which is a dramatic difference of dozens of times. Also, in the Hong Kong outbreak, 90% of those who died were elderly people.
From these two examples, two conclusions can be drawn. The first is that vaccines are highly effective at preventing severe illness and death. In Yangzhou, the vaccines used were mainly produced on the mainland. In Hong Kong, mRNA vaccines and inactivated vaccines were mainly used, accounting for about 60% and 40%, respectively. The second is that, the elderly and people with underlying diseases are the most in need of protection and vaccination. I think two conclusions can be drawn from these two examples.
Therefore, in order to further increase vaccination rate among the elderly, the next step is to scale up publicity and mobilization in two aspects. For one thing, we should raise their awareness. We must not only emphasize the principle of vaccination on a voluntary basis, but also emphasize the sense of responsibility. We often say that one should hold the primary responsibility for his or her own health. In the context of the pandemic, vaccination is not only to protect oneself, but also to protect the family, and to contribute to society. For another, we must also actively respond to the concerns of the elderly. Why do the elderly have so many concerns and worries? Why do they lack the motivation to receive vaccinations? It is necessary to figure out the causes and respond to their concerns and questions. For example, how about the safety of vaccines, which is something the elderly are concerned about. What are the side effects, and how is vaccine efficacy? How about the protective effect on the elderly? Will vaccination aggravate underlying diseases? Given that many elderly people have underlying diseases, will they get worse after being vaccinated? There are also elderly people who think that they don't leave their homes frequently and so wonder if it's necessary to get vaccinated? Only when we bring clarity to their unease can we encourage them to get vaccinated. Therefore, relevant units and experts must attach great importance to informing the public about data and relevant information. The media should spread relevant information widely in a way that the elderly like to see. In these ways, the whole of society works together to form a favorable environment that is conducive to increasing the vaccination rate among the elderly.
Second, we should give full play to the role of local relevant departments. Grid management systems can be employed to enable the elderly to get vaccinated. Relevant departments can also actively mobilize key groups such as the elderly and key places such as nursing homes so as to increase the vaccination rate among the elderly.
Third, we should ensure the safety of the elderly getting vaccinated. The vaccination unit should arrange for medical staff who are familiar with the physical condition and the diagnosis and treatment of diseases of the elderly to stand by to provide health care. Before an elderly person gets vaccinated, the medical staff should carry out health assessments on them. After the vaccination, the healthcare professionals should carry out surveillance of the vaccine recipients for signs of adverse events and be particularly prepared for an emergency. Because the elderly may have underlying health conditions, we must ensure prompt and proper medical treatment in case of emergencies.
Fourth, more convenient measures should be taken to facilitate vaccination among the elderly. Mobile vaccination vehicles and other equipment can be used to set up temporary vaccination sites to shorten their round-trip route. Housecalls can also be made for those having difficulty getting about, and more green channels can be set up to shorten the waiting time for old people. We should also make flexible arrangements at vaccination spots according to their demands. By implementing such measures, we believe that the vaccination rate among the elderly is sure to rise soon. Thank you!
_ueditor_page_break_tag_
Thecover.cn:
According to a document recently released by the State Council joint epidemic prevention and control mechanism, residents can buy antigen COVID-19 test kits themselves as an additional test method to nucleic acid tests. Do the self-purchased test kits need to be put on record? If a positive test result is not reported, are there any corresponding regulatory measures?
Jiao Yahui:
Thank you for your questions. First of all, residents buying antigen COVID-19 test kits do not need to be put on record. As stipulated in the antigen testing plan, anyone who tests positive using the self-test kits should report the results to their community, and the community will arrange a special vehicle to transport the case to a medical institution for further nucleic acid testing for confirmation. The whole process is a closed loop. The State Council joint prevention and control mechanism has made specific regulations for all localities to make detailed arrangements for the discovery, report and closed-loop management of cases. Provinces have been required to clarify their detailed plans.
Just now, you mentioned whether the reporting of self-tested positive results needs supervision or not. I'd like to remind the general public: on the one hand, as Mr. Zeng has explained, everyone is the first person responsible for their own health as well as the health of their families. On the other hand, the pandemic prevention and control regulations stress responsibilities from four aspects, of which one is personal responsibility. Therefore, we call for timely reporting if a positive result is found through the use of a self-testing kit. In addition, the Law on Prevention and Treatment of Infectious Diseases and other laws and regulations also clearly stipulate that citizens have the responsibility and obligation to report a positive case, and if they violate the rules and cause the spread of infectious disease, they should shoulder the corresponding legal liability.
In our practice of epidemic prevention and control, we can see that some violators in many places have been investigated for legal liability. So, I'd like to remind the public that if they test positive, they should first report it according to the local requirements.
Shou Xiaoli:
Due to time constraints, we'll take one last question.
_ueditor_page_break_tag_
China News Service:
Recently, China has seen frequent flare-ups of COVID-19 cases in multiple places, with a large swathe of areas affected. Locally transmitted cases and cluster infections have been reported in a number of provinces. Given the circumstances, what suggestions do you have for strengthening personal precautions? Thank you.
Wang Hesheng:
Thank you. I'm glad to take this question. In my opinion, we need to remind people to strengthen personal precautions throughout every stage of COVID-19 response, not just when the epidemic situation is severe. We need to step up self-protection both when there is no significant resurgence and amid routine epidemic prevention and control. I would like to offer a few suggestions.
First, I would like to continue with the issue of vaccination for senior citizens that Mr. Zeng mentioned earlier. I believe that boosting vaccination and strengthening personal precautions should be the top priority. According to classic theories of infectious disease, controlling the sources of infection, cutting off transmission routes, and protecting vulnerable groups are the top three methods of prevention and control. In this sense, vaccines are the most effective ways to protect vulnerable groups. Vaccination has seen remarkable results based on our practices, especially among senior citizens. The COVID-19 resurgence in Hong Kong is a poignant lesson for us, and the situation proves that a low vaccination rate among the elderly will lead to a high mortality rate. A question raised just now also mentioned that some senior citizens didn't get vaccinated because they thought they rarely went out, which was inconvenient in nursing homes.
Nevertheless, please remember that the vaccinated and unvaccinated will face utterly different consequences once infected, and what happened in Hong Kong is an example. Therefore, while we all treat the elderly with respect and strive to be role models in this regard, we must encourage our senior family members to get vaccinated because they most need personal precautions. China has provided extraordinary vaccines and inoculation services, and every sector is proactively working to implement the work. As far as I know, China's civil affairs departments have made plenty of effort to step up collective prevention and control in nursing homes. This is because many senior citizens also understand the importance of vaccination and are actively applying for inoculation. Therefore, departments associated with vaccines and civil affairs government bodies should work closely together and provide good services for these senior citizens following relevant requirements. All of these are my first-hand experience. We need first of all to make better use of vaccines to strengthen epidemic prevention.
Second, we need to maintain good personal hygiene habits. We have gained good experience after this long epidemic. When staying at home, we need to enhance ventilation and disinfection and maintain personal hygiene. When going outdoors, we must wear face masks, strengthen personal precautions, and keep our hands clean. We also need to practice social distancing and avoid crowded places, gatherings, and group dining activities.
Third, we should do our part in implementing the requirements of COVID-19 response. We should proactively assist in the epidemiological investigation and nucleic acid tests, especially in public spaces' prevention and control requirements. There are many anti-virus requirements in public areas, and we must refrain from acting willfully, playing petty tricks, or refusing to scan health QR codes and follow relevant rules. Cooperating with anti-epidemic work is essential, and it is good to all of us.
In addition, we need to pay close attention to our health status. We must seek medical help and report to the community promptly in case of fever and dry cough. Let's work together to establish a solid society-wide defense line. Thank you.
Shou Xiaoli:
Thank you to all three speakers and friends from the media. Today's press conference is at this moment concluded. Goodbye.
Translated and edited by Zhang Liying, Li Huiru, Li Xiao, Zhang Rui, Cui Can, Wang Wei, Liu Sitong, Yang Xi, Zhang Junmian, Xu Xiaoxuan, Huang Shan, Zhu Bochen, Liu Qiang, Chen Xia, Qin Qi, Yuan Fang, Zhang Tingting, Wang Yiming, David Ball, Jay Birbeck and Tom Arnstein. In case of any discrepancy between the English and Chinese texts, the Chinese version is deemed to prevail.